Most teams have a publication strategy. Very few have one for what happens after publication. We turn the paper you already earned into a story physicians finish, and a journey each reader steers. Nothing new is created, and it is built for MLR from the first frame.






The same approved paper lands on two very different desks. Tap a physician and watch their route through it change. Neither one sits through the other’s part.

Same paper, two reads, one review. The routes recombine approved modules, so no new claims are ever created and one MLR review covers every journey. That is what a publication becomes here: not one video for everyone, a way in for each reader.
The science is done. Making it perform is the problem. Publication took years, and then the reading stops at the abstract.
The subgroup analysis your team fought to include? Never seen.
Most of the time, the abstract is where the reading stops.
of HCPs are unreachable through conventional digital outreach.
percent of pharma teams believe their outreach works. Twenty-eight percent of physicians agree.
Nothing about your evidence changes. Everything about how it travels does.
Pick a section of the publication and see the scene it becomes, one the reader can open, not just look at. The structure you approved is the structure that plays.
The Impact Gap Report 2026 · free. That number, next to 60 more like it, and what the evidence says actually gets read.
See the whole picture →
Bring the paper you already have. You bring the publication and the therapeutic-area context. We do the heavy lifting.
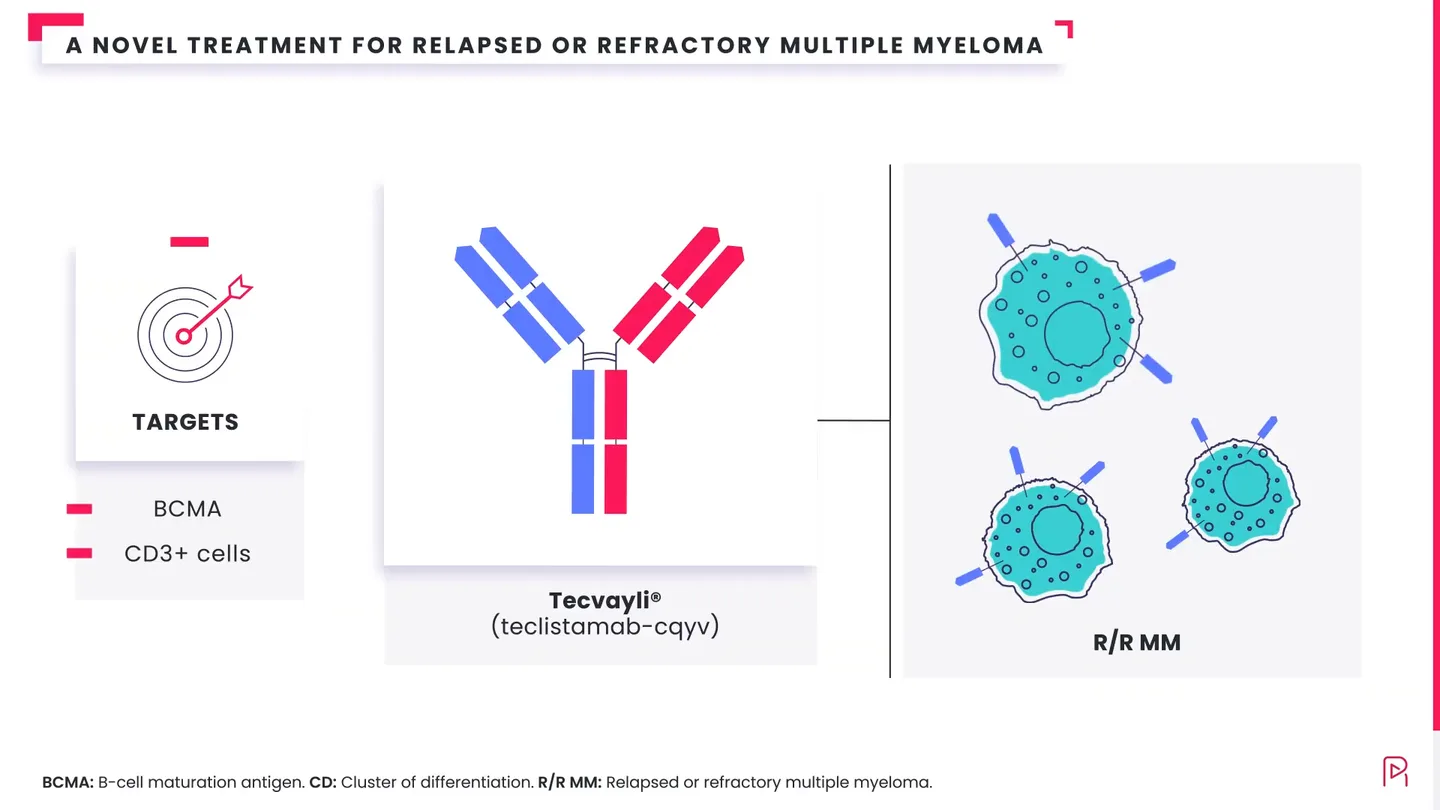
2:10The molecule and its target, shown in motion instead of described in a caption.
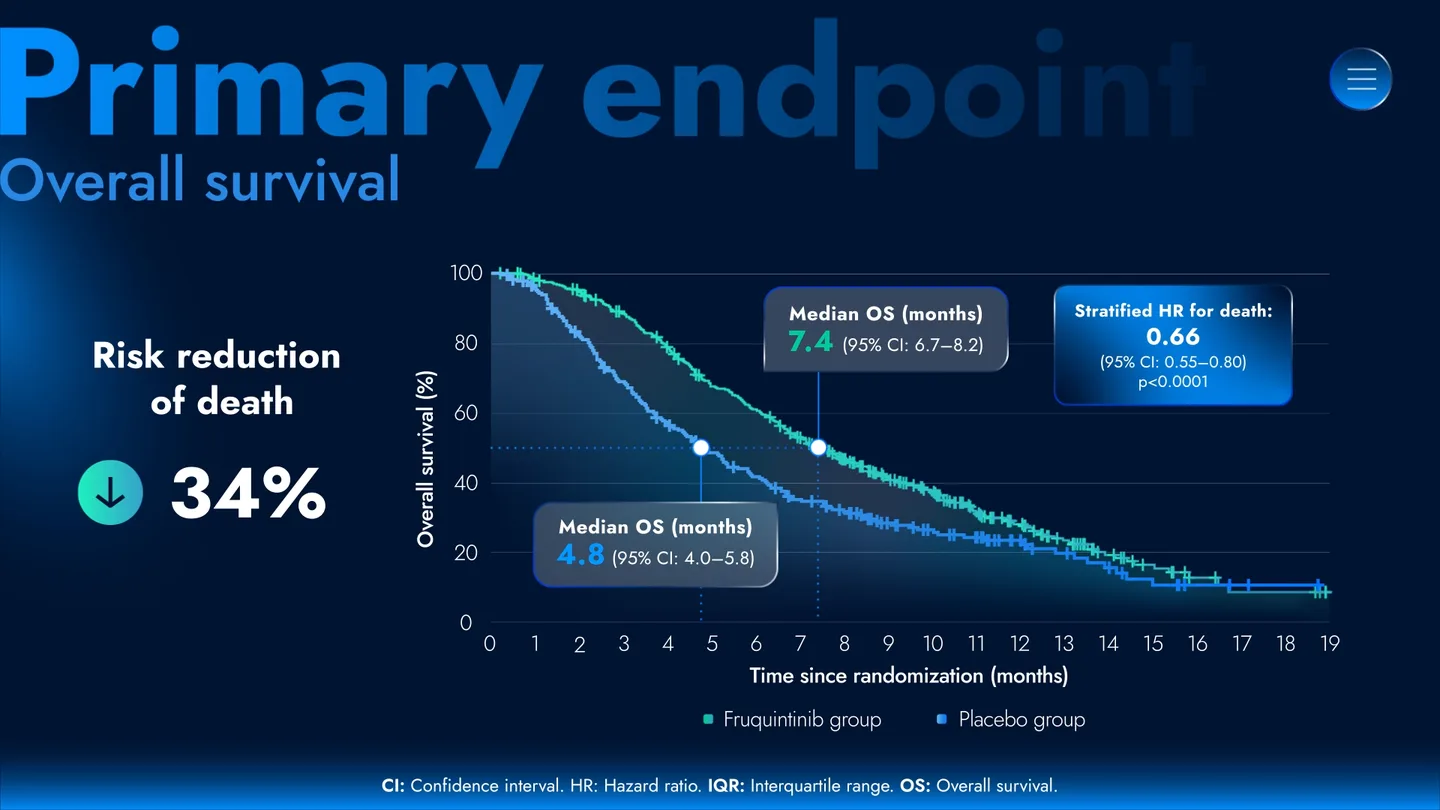
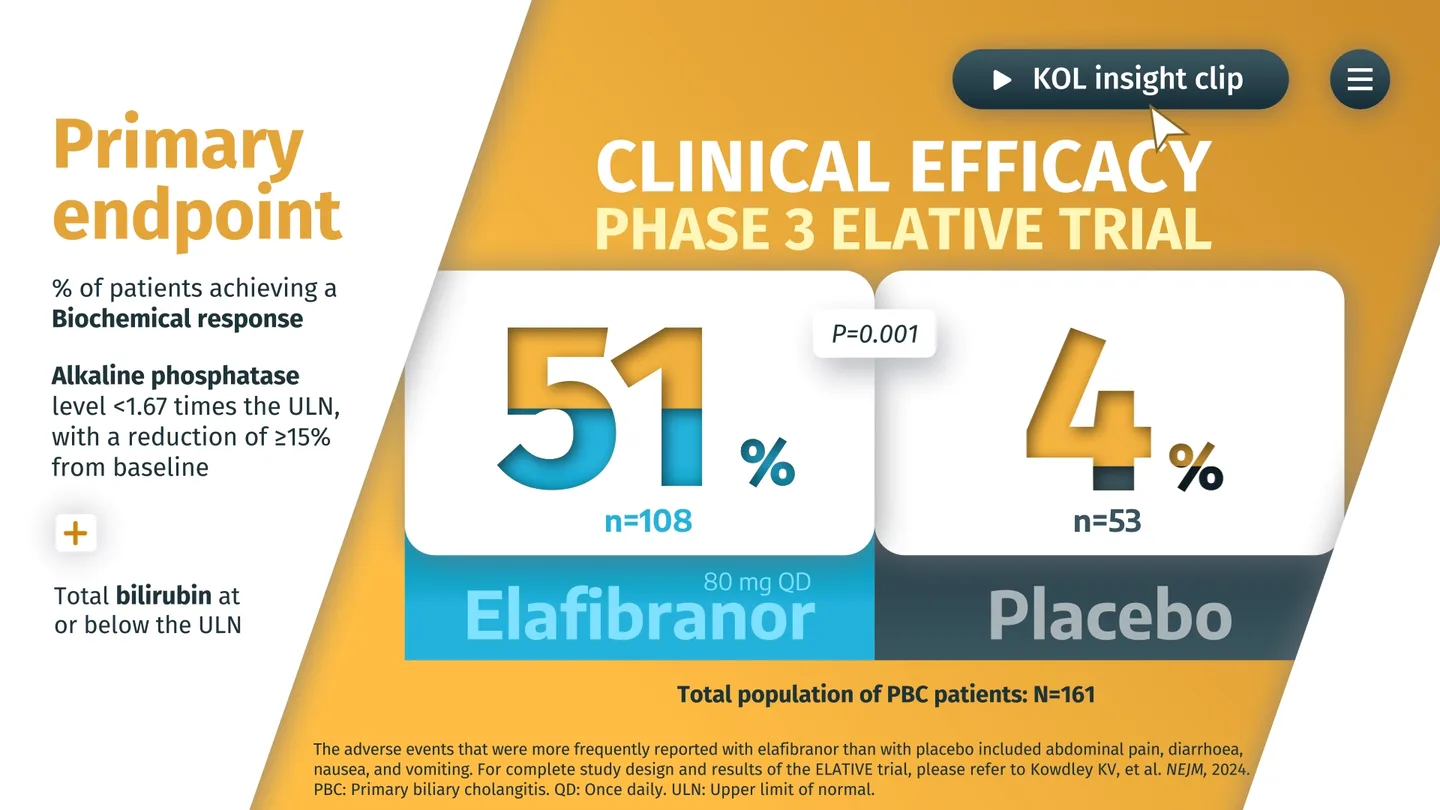
1:48The primary endpoint drawn so the result lands before the physician looks away.
2:22How the finding holds up in everyday practice, kept current as data grows.
 1:36
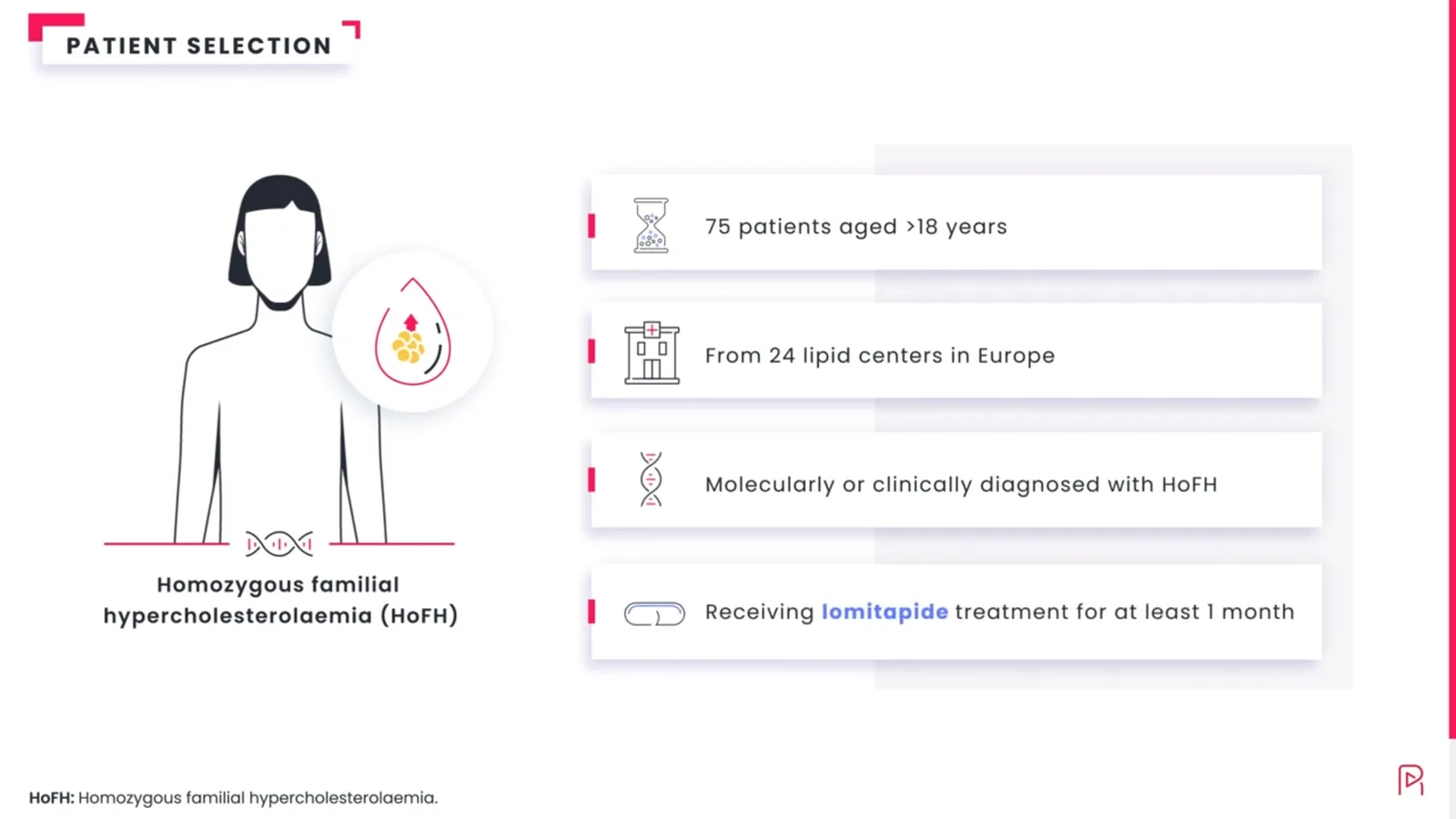
1:36The unmet need behind the study, made concrete before the data arrives.
 0:40
0:40The whole publication stays linked, for the physician who wants every detail.
 0:52
0:52Every claim tied to its source, checkable without leaving the screen.
Every frame maps back to the approved source. No claim appears that was not already in the publication, so it is built for MLR from the first frame and drops into your existing Veeva workflow.
One approved core becomes every language and every market you need, without starting the science over each time.
“It is the first format my MSLs say physicians actually finish.”
Send the paper. We will come back with how we would approach it: the two-minute story, and where the journeys would split for your readers. On the house. No promises. If it is not right, you keep the thinking.
The video is the way in. On top of it, physicians explore the sections they care about, the story adapts to what each physician explores, and smart nuggets turn interest into an approved next step, mid-story. A video gets watched once; this keeps working after the first play.
No. Every frame maps to a claim already in your approved publication. We change the delivery, never the science, which is what keeps it structured for review from the first frame.
The published paper and the therapeutic-area context. You bring the evidence you already earned; we do the mapping and the build.
We will not tie it to a fixed date. You approve the core the normal way, at script, storyboard, and final animation. From there, that same approved core carries every version, so new cuts and languages do not restart the scientific review. The overall pace tracks your own review, which we plan around with you from day one.
Always. The experience is the way in, not a replacement. The complete publication and every reference stay one tap away for the physician who wants all of it.
Yes. One approved core is produced in 30+ languages without rebuilding the science each time, and the review you ran carries across them.