Every reader opens your readout with a different question. The outcomes physician wants the curve. The community cardiologist wants to know if it holds up in her clinic. A film that answers in one fixed order loses most of them. This one answers each of them first. Try it on the right.
You just did what physicians do. Straight to the part you cared about, skipped the rest. That is the read we build for.





A clinical trial animation that only plays is still a monologue. It answers every reader in the same fixed order, and most of them stop before their answer arrives.
Nearly half of physicians never see it through the channels you have.
percent of pharma teams believe their outreach lands. Twenty-eight percent of physicians agree.
of the time, physicians read only the abstract, not the results underneath.
One approved readout, built so the physician steers the read. The conclusion is the same for everyone. The route there is their own.
The same approved readout lands on two very different desks. Tap a physician and watch the read change. The trialist goes straight to the curve; the community cardiologist reads whether it holds for the older patients in her clinic. One readout, one review.

60+ studies on why physicians stopped reading pharma’s science, and the evidence for what works instead. Sourced, quotable, built for forwarding.
Get it now · free →
Bring the paper, the poster, or the topline. You bring the data and the context. We do the heavy lifting.
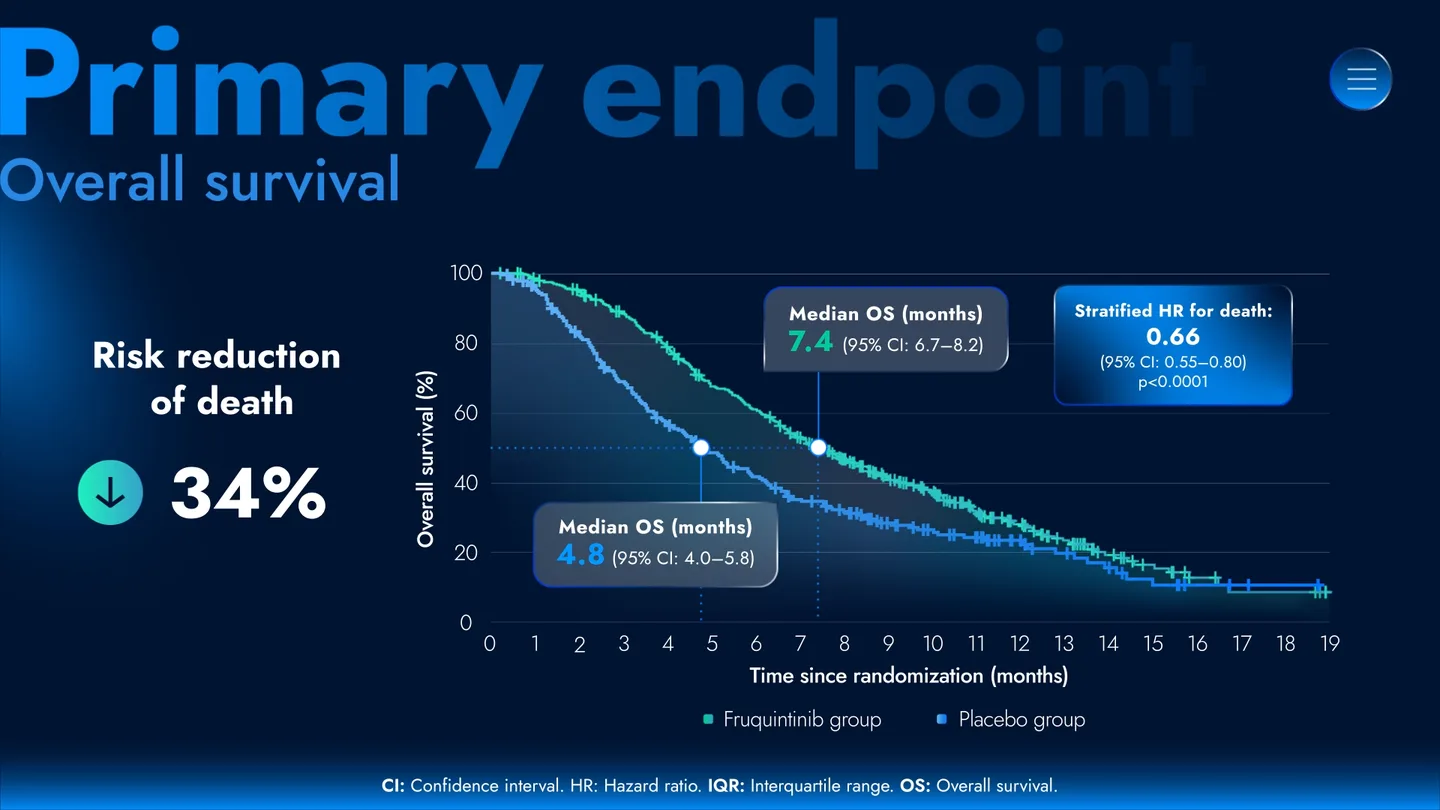
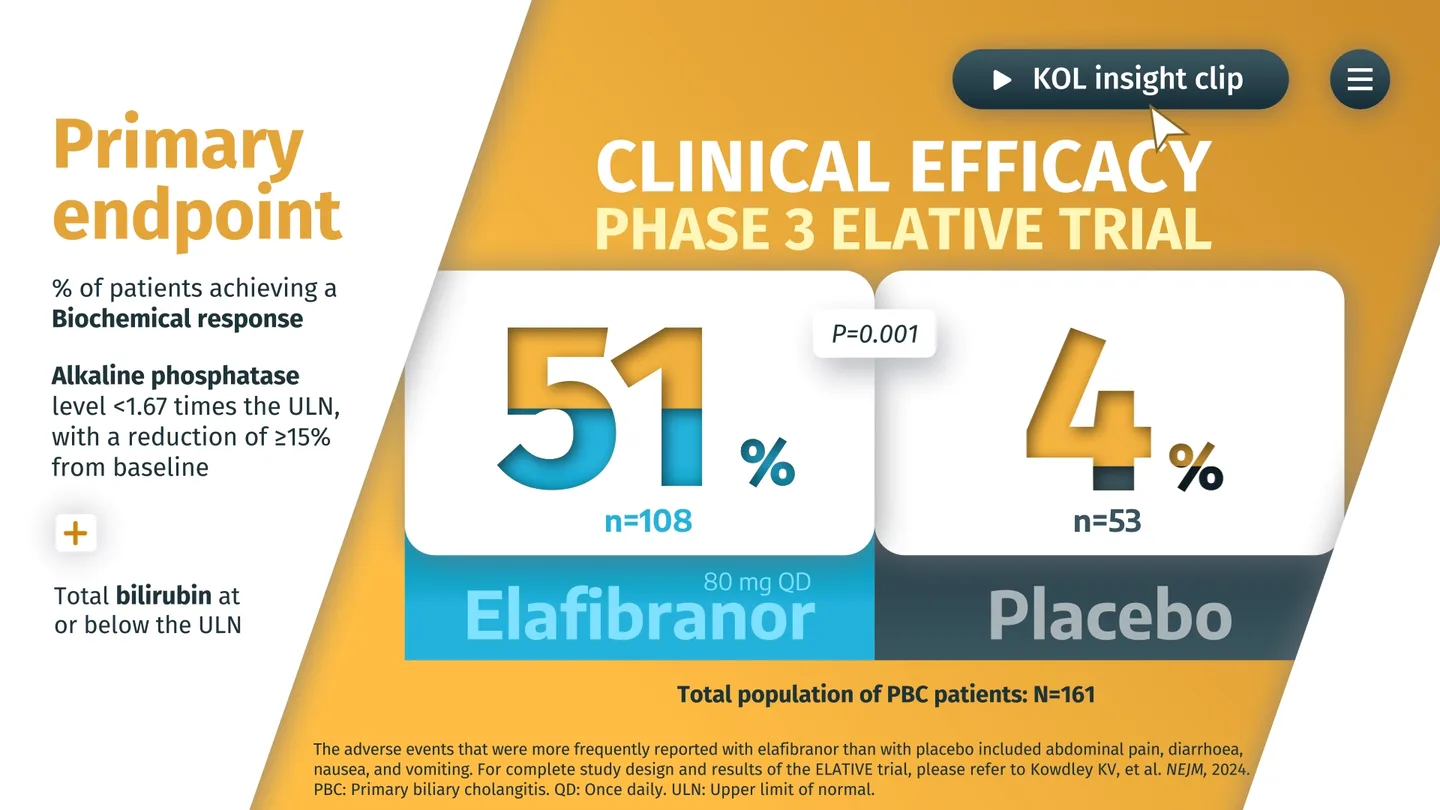
1:48The curve or the number, drawn so the finding reads in a single look.
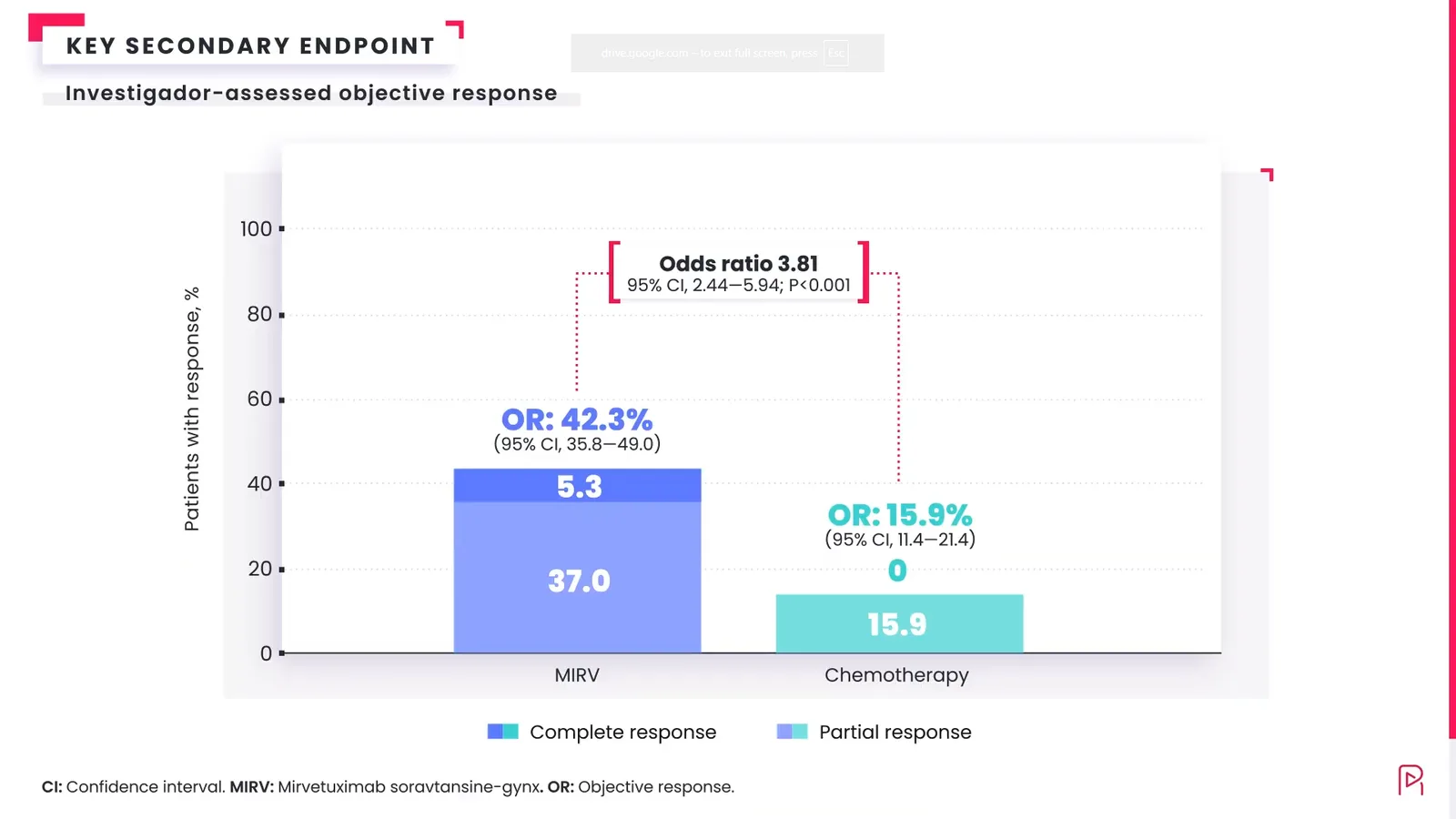
2:06Who benefits and by how much, kept honest and kept in proportion.
1:34The safety profile shown in sequence, not buried in the last table.
 2:20
2:20How the trial finding holds up in everyday practice, kept current.
We do not round up, smooth over, or add a number that was not in the readout. Every frame maps to the trial data you approved, so it is built for MLR from the first frame.
“They watched the safety section. That never happened with the slides.”
Send the paper, the poster, or the topline. We will show you how physicians would explore it, endpoint by endpoint. On the house. No promises.
Both. It plays on its own for the reader with 30 seconds, and it opens up for the one who wants every endpoint. With PubVisual Engage on top, interest becomes an approved next step inside the story: ask a question, request the paper, book time.
No. We change the order and pace of the read, never the numbers. Every frame maps to the trial data you approved, which is what keeps it built for MLR.
Yes. A published paper, a congress poster, or a topline readout all work as a starting point. Bring the data and the context; we build the story.
As part of the story, in sequence, not as the slide nobody reaches. The full profile is shown honestly and kept in proportion to the rest of the readout.
We will not tie it to a fixed date. You approve the core the normal way, at script, storyboard, and final animation. From there, that same approved core carries every version, so new cuts and languages do not restart the scientific review. The overall pace tracks your own review, which we plan around with you from day one.
It is built for it. Because every frame traces to an approved data point, the animation is structured for MLR from the first frame and fits your existing Veeva workflow.