Medical animation, and scientific animation more broadly, only earns its cost when the physician can explore the part that matters to them. We turn your approved science into a scene they steer at their own depth, from mechanism of action to trial data, built for MLR from the first frame. The animation is not the goal. Understanding is.
Medical animation and scientific animation cover the same craft: turning approved data into something a physician can see and steer. But not every story needs 3D, and a slick render nobody finishes is a cost, not an asset. We build the format the science actually calls for, and every frame maps to an approved reference, structured for MLR from the first frame.
Bring us the publication and the therapeutic area. We do the heavy lifting: the mapping, the modeling, and the interactive build around it. Here is where each format fits.






On the left, the mechanism as a slide asks the physician to picture the motion. As a scene, the motion is already there. Watch it switch.
The same approved animation serves the generalist who needs the gist and the specialist who wants the molecular detail. Pick a depth and watch the same mechanism meet it.
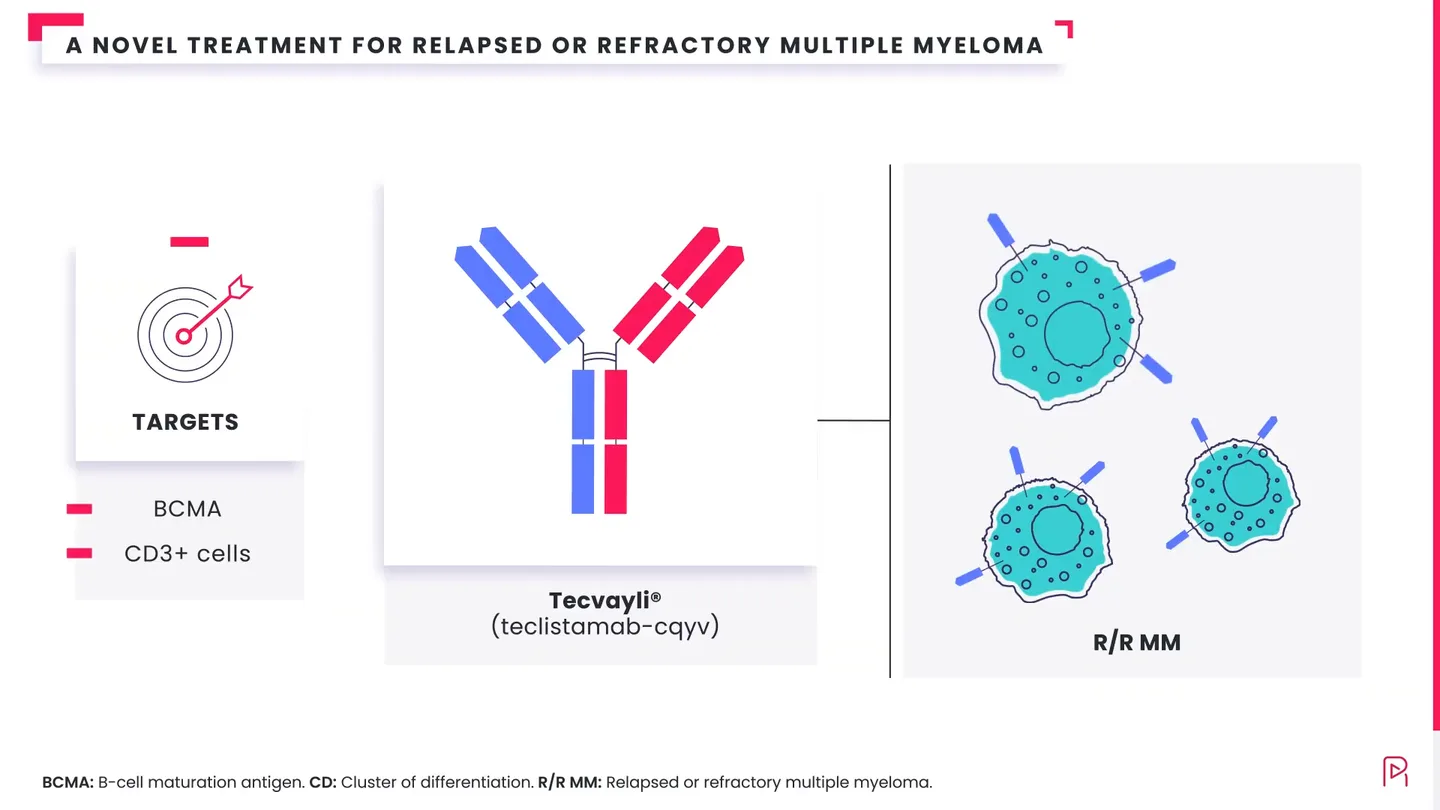
The molecule binds its target and switches the pathway off. That is the takeaway, and for a lot of physicians it is all they need before they move on.
The same approved animation lands on two very different desks. Tap a physician and watch their route through it change. One follows the binding step by step; the other needs only what it means at the bedside. Neither sits through the other’s part, and it is all one MLR review.
The Impact Gap Report 2026 · free. That number, next to 60 more like it, and what the evidence says actually gets read.
See the whole picture →
Small molecule, biologic, cell therapy, vaccine. You bring the science and the target. We do the heavy lifting.
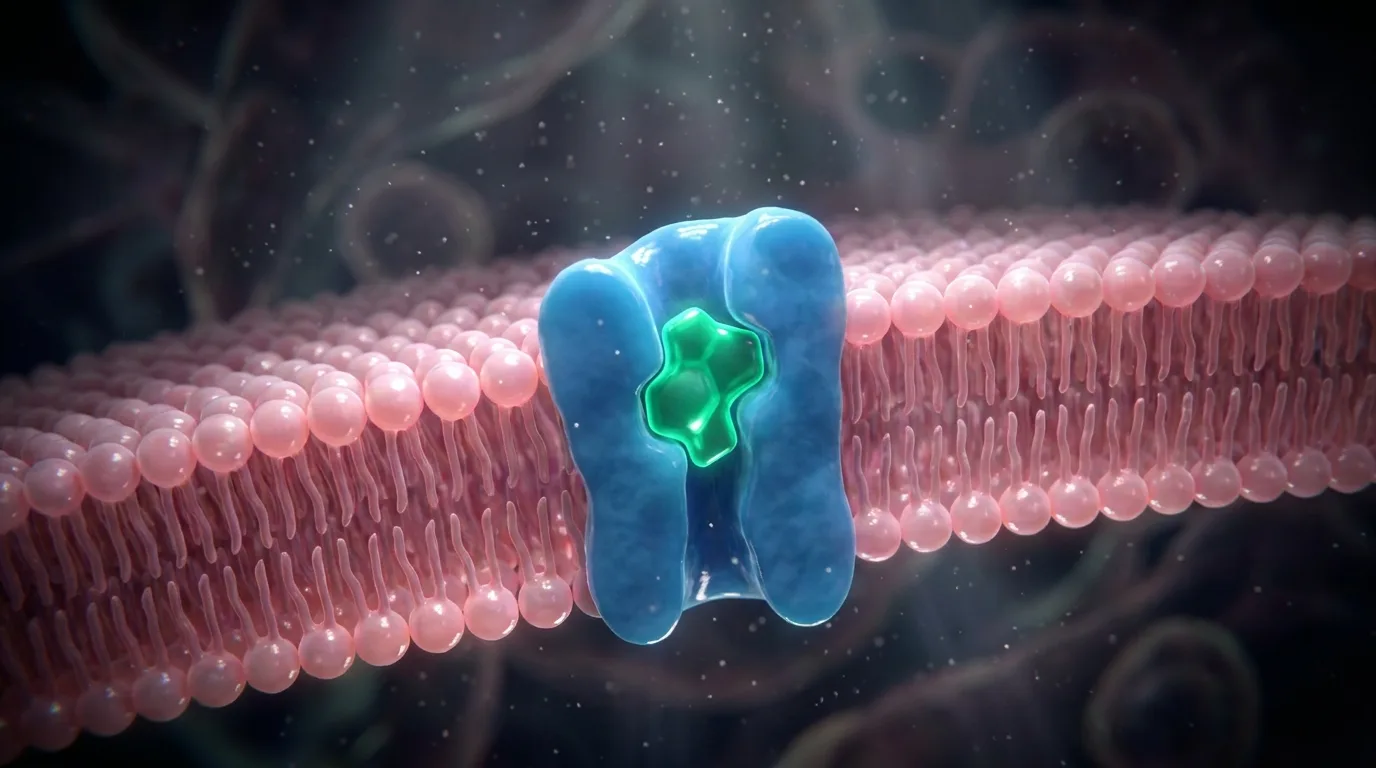
2:04How the molecule finds and binds its target, at the scale it happens.
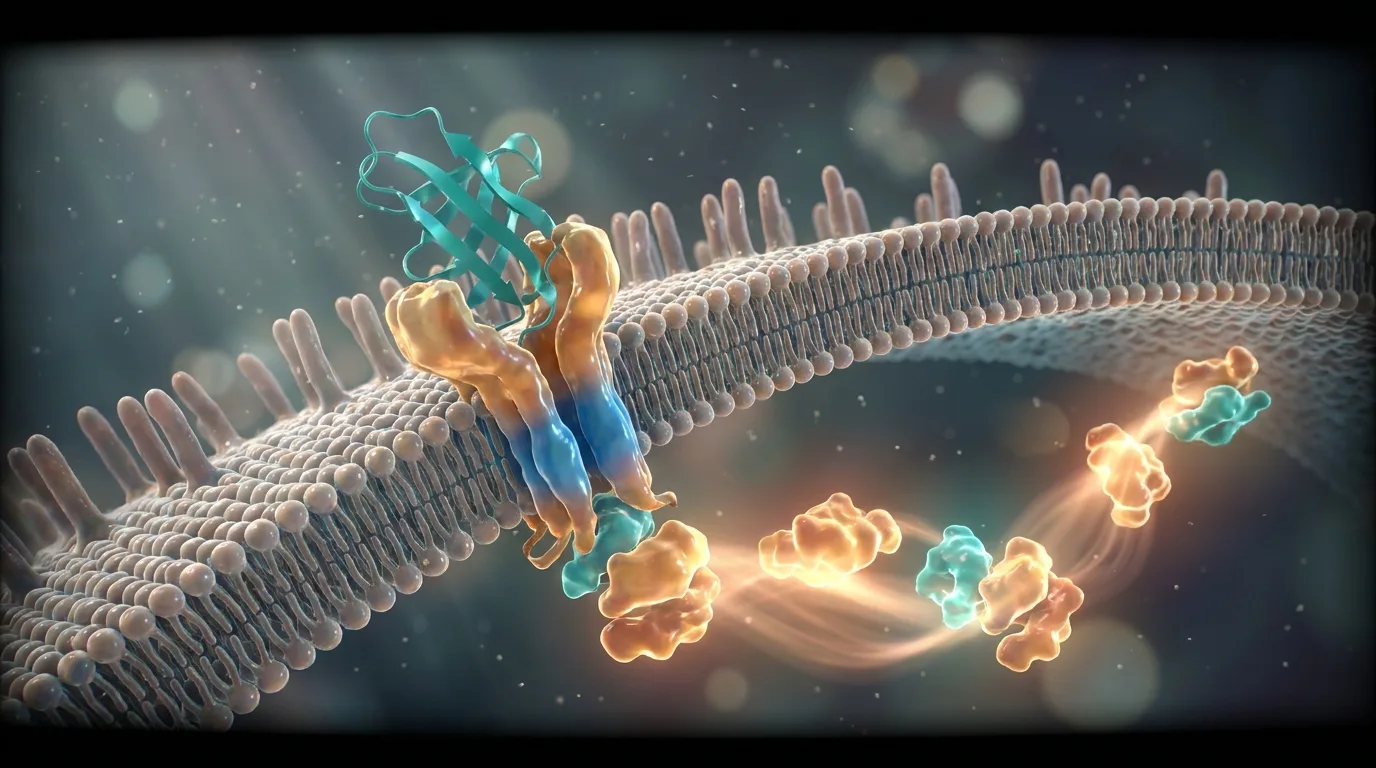
1:52The pathway that follows, shown step by step instead of stacked on one slide.
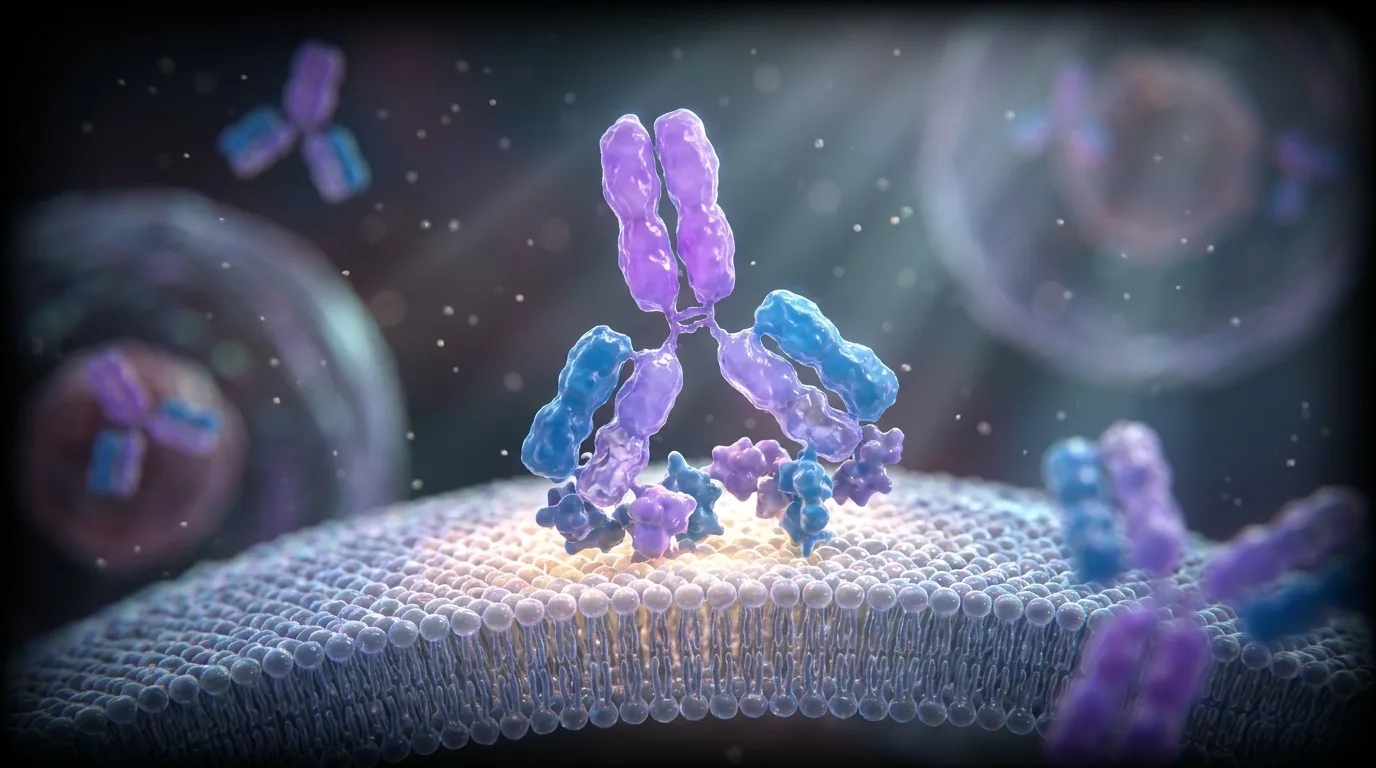
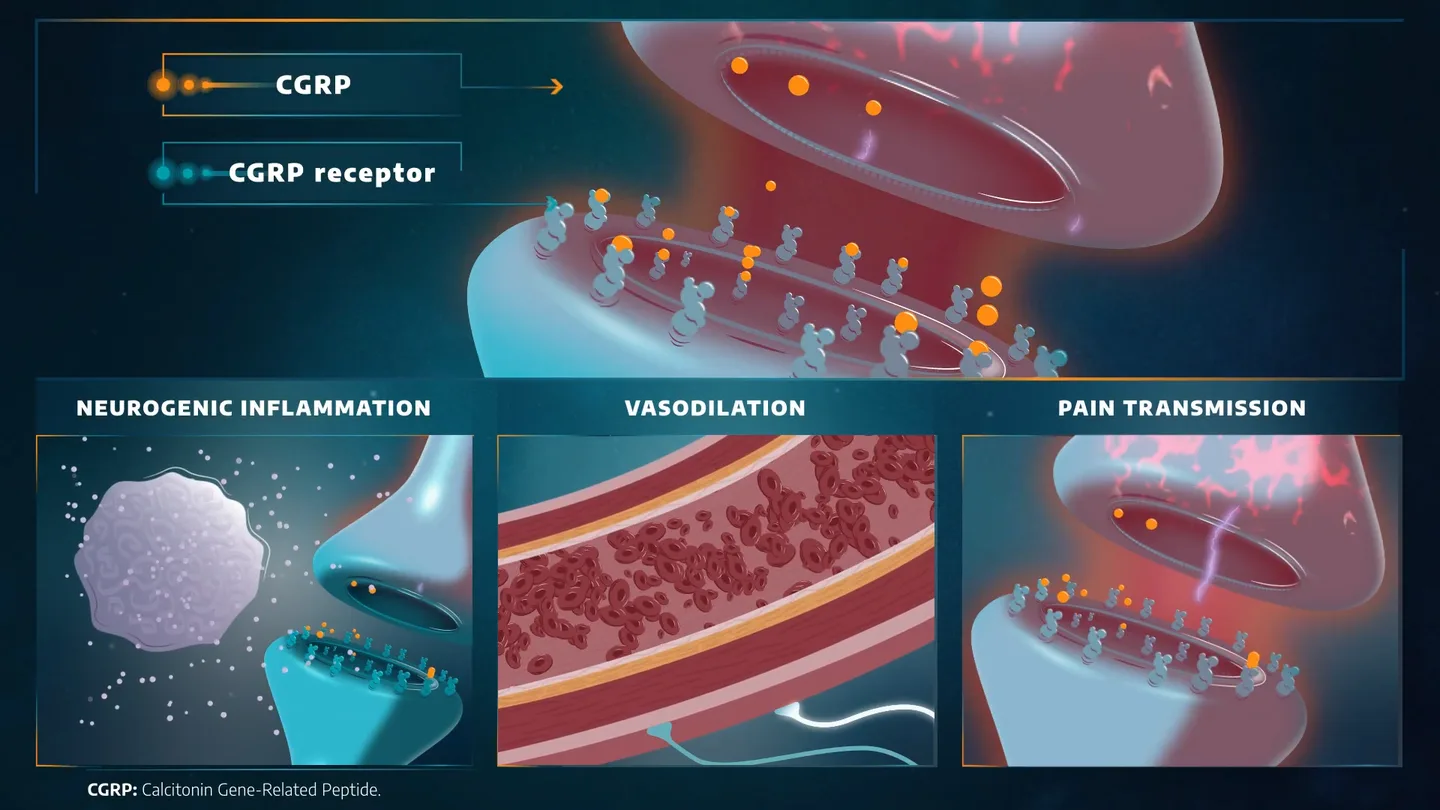
2:18The synapse forming, the response starting, the interaction made visible.
 1:36
1:36Why a mechanism stops working, so the next step in the story makes sense.
We change how it is shown, never what it says. Every element maps to your source, so the animation is built for MLR from the first frame.
One approved core carries into every market and language you serve, without rebuilding the biology each time.
“They did not just watch it. The registrar went two levels deeper on her own.”
Send the figure and the paper it came from. We will show you the scene it becomes and how a physician would explore it, at their depth. On the house. No promises.
In practice they are the same craft: turning approved data into something a physician can watch and explore. "Medical animation" tends to describe clinical and mechanism content for HCPs and patients; "scientific animation" is the broader term for any data or process made visual. We build both from your approved science, structured for MLR.
It depends on whether the shape or motion is the point. 3D suits structure, binding, and cascades; a clean interactive sequence suits most trial data, value stories, and comparisons. We tell you which one your science actually needs rather than defaulting to the most expensive render.
Yes, that is the usual starting point. Bring the figure and the source it came from; we map it, model it, and set it in motion.
Anywhere the mechanism needs to be understood: a standalone film, a congress screen, a rep’s tablet, or inside a larger interactive story. One approved core, many placements.
We will not tie it to a fixed date. You approve the core the normal way, at script, storyboard, and final animation. From there, that same approved core carries every version, so new cuts and languages do not restart the scientific review. The overall pace tracks your own review, which we plan around with you from day one.
Yes. Because every element traces to an approved claim, it is structured for MLR from the first frame and fits your existing Veeva workflow.