A beautiful render gets watched once and forgotten. Your science performs when the physician can reach the part that matters to them, in their own time. That is the upgrade. Not more polygons.





The physician does not remember the render. They remember whether they understood, and whether they could get to the part that mattered to them. So we build for that first, and we use 3D only where it earns its place.
The same 3D scene, three different questions. Press into the one you would want to see. This is what your physicians do with it, no login, no download.
A render everyone watches shows all of them the same thing, in the same order. Tap a marker and see what happens when the physician gets to steer instead.
You just did what a physician does. You went straight to the part you cared about and skipped the rest. A render they can drive is the one they remember, because they built the memory themselves.
The same approved render lands on two very different desks. Tap a physician and watch how far into it they go. The specialist turns it over from every angle; the generalist takes the one-line version. Same render, one review.

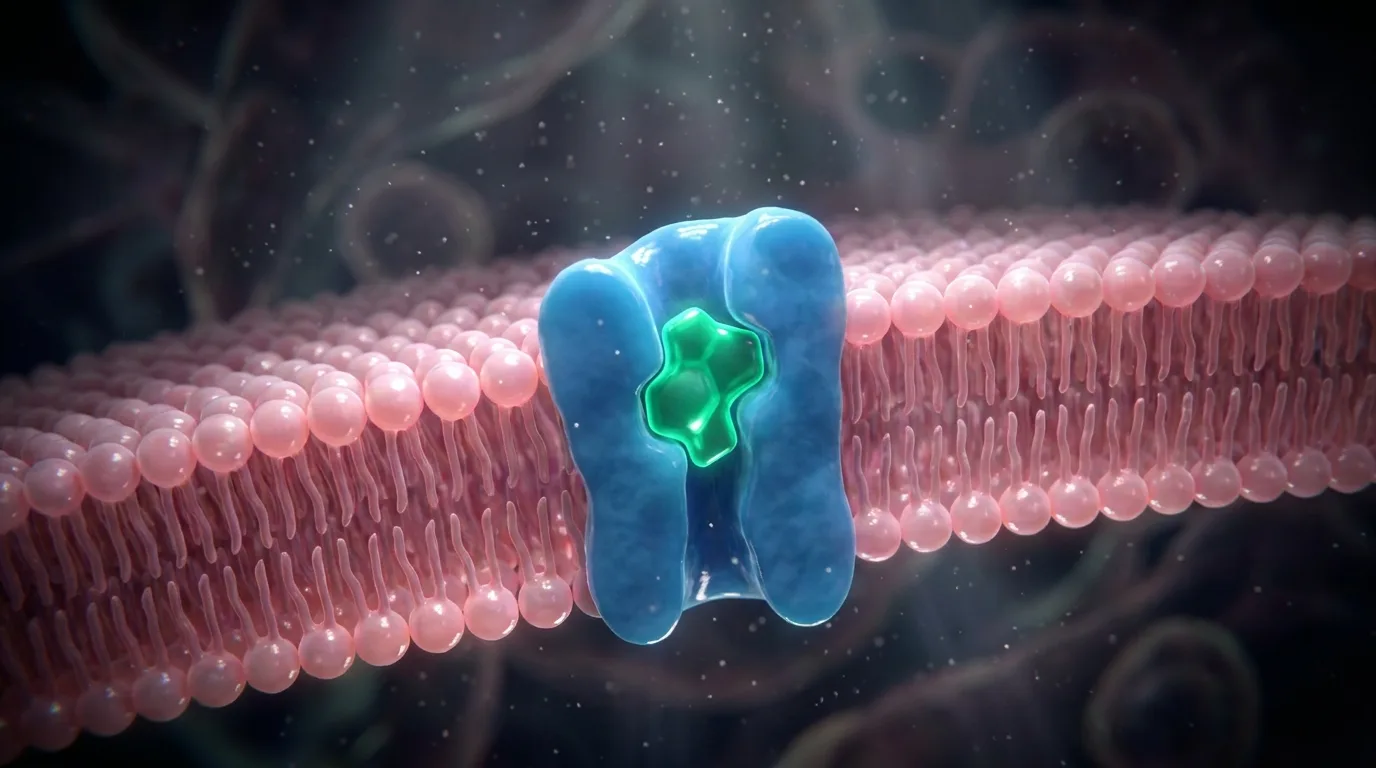
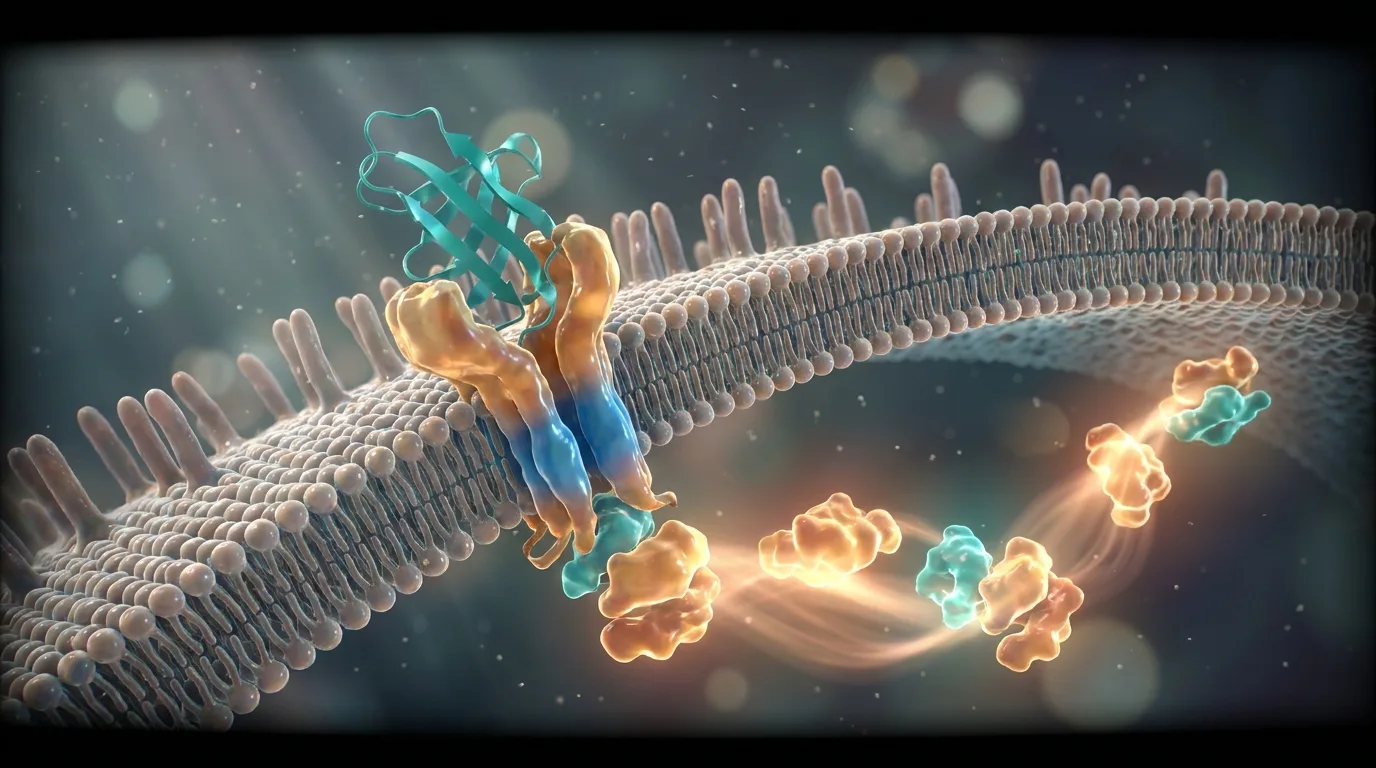
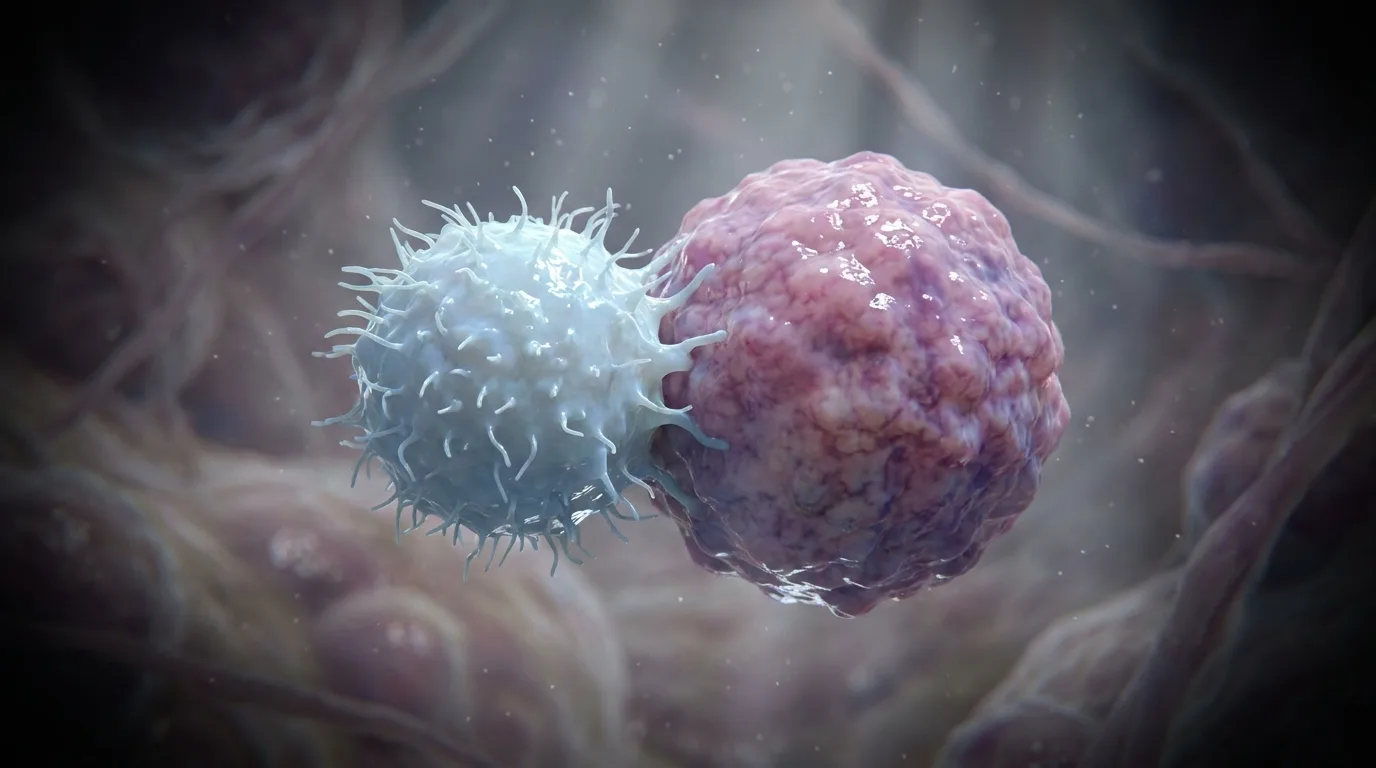
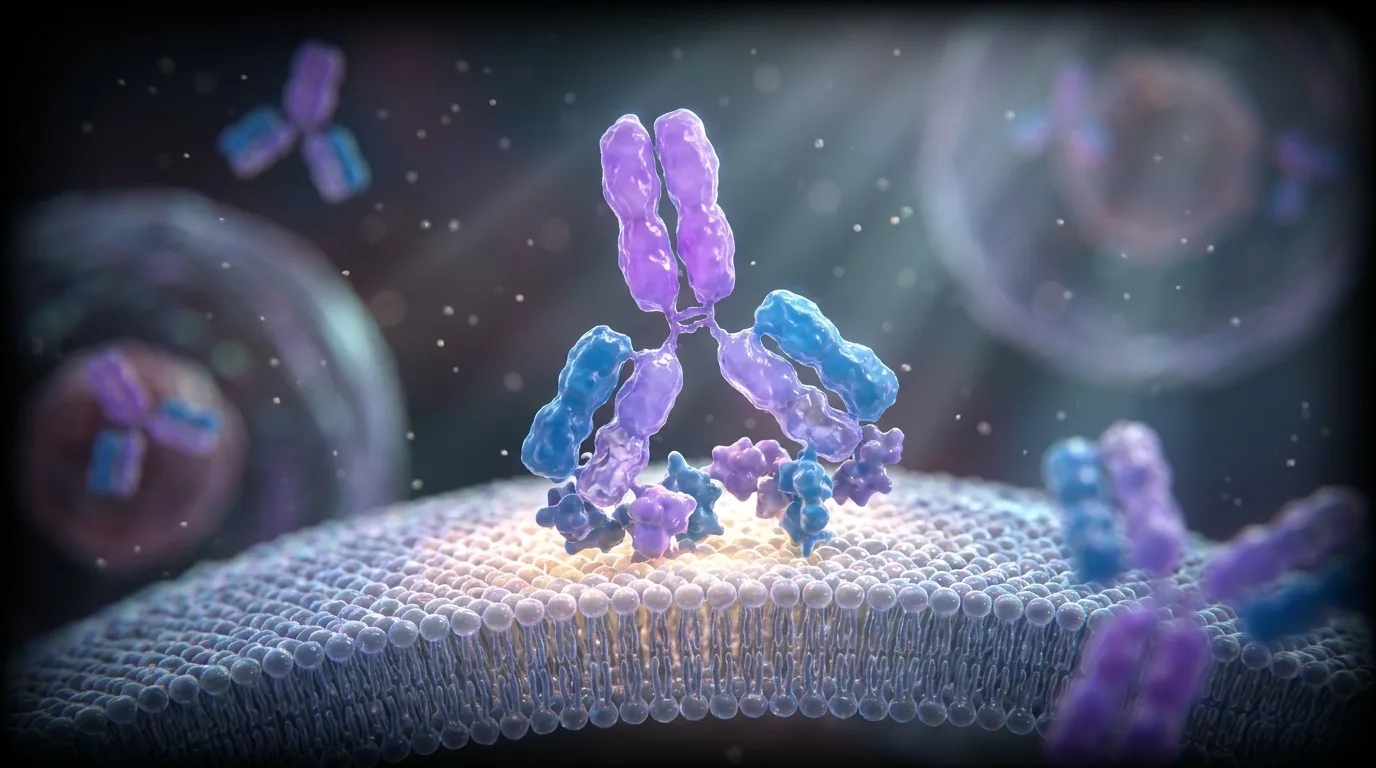
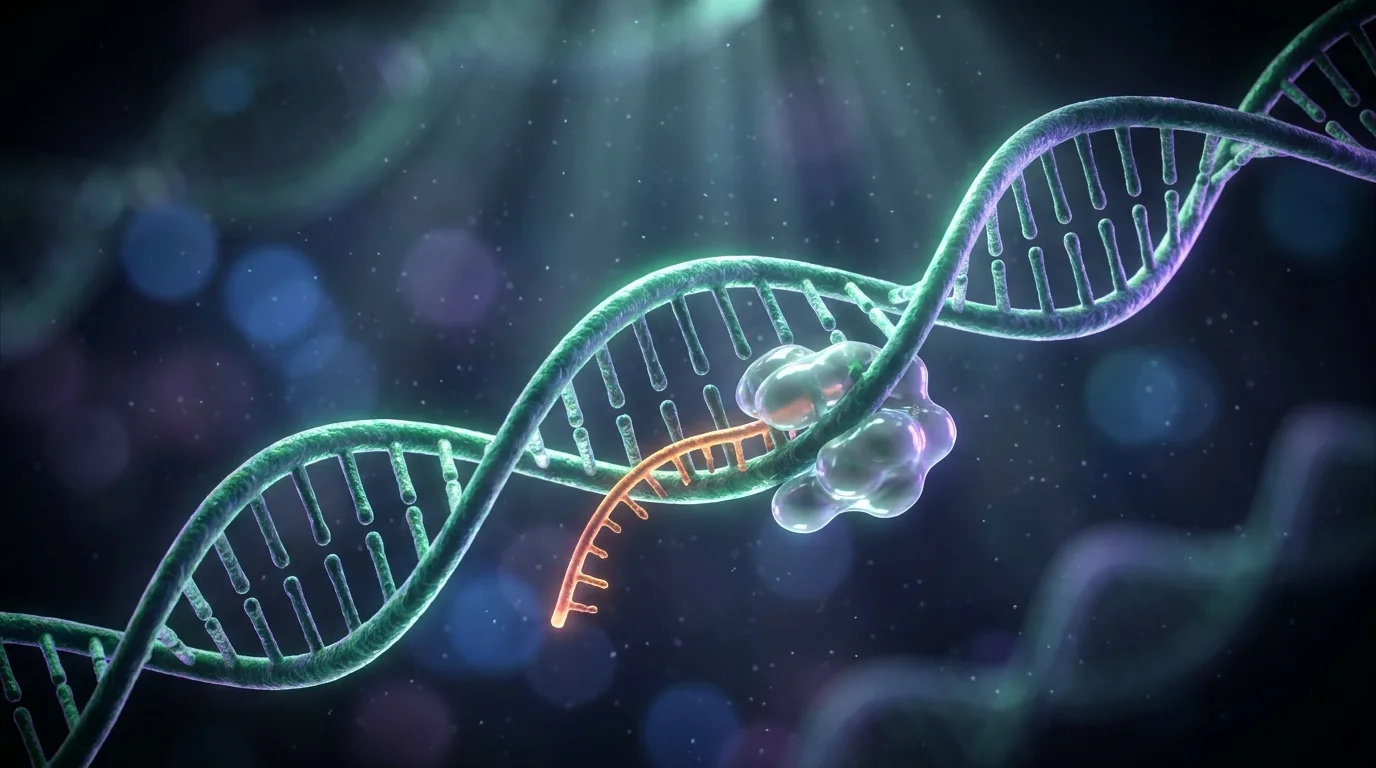
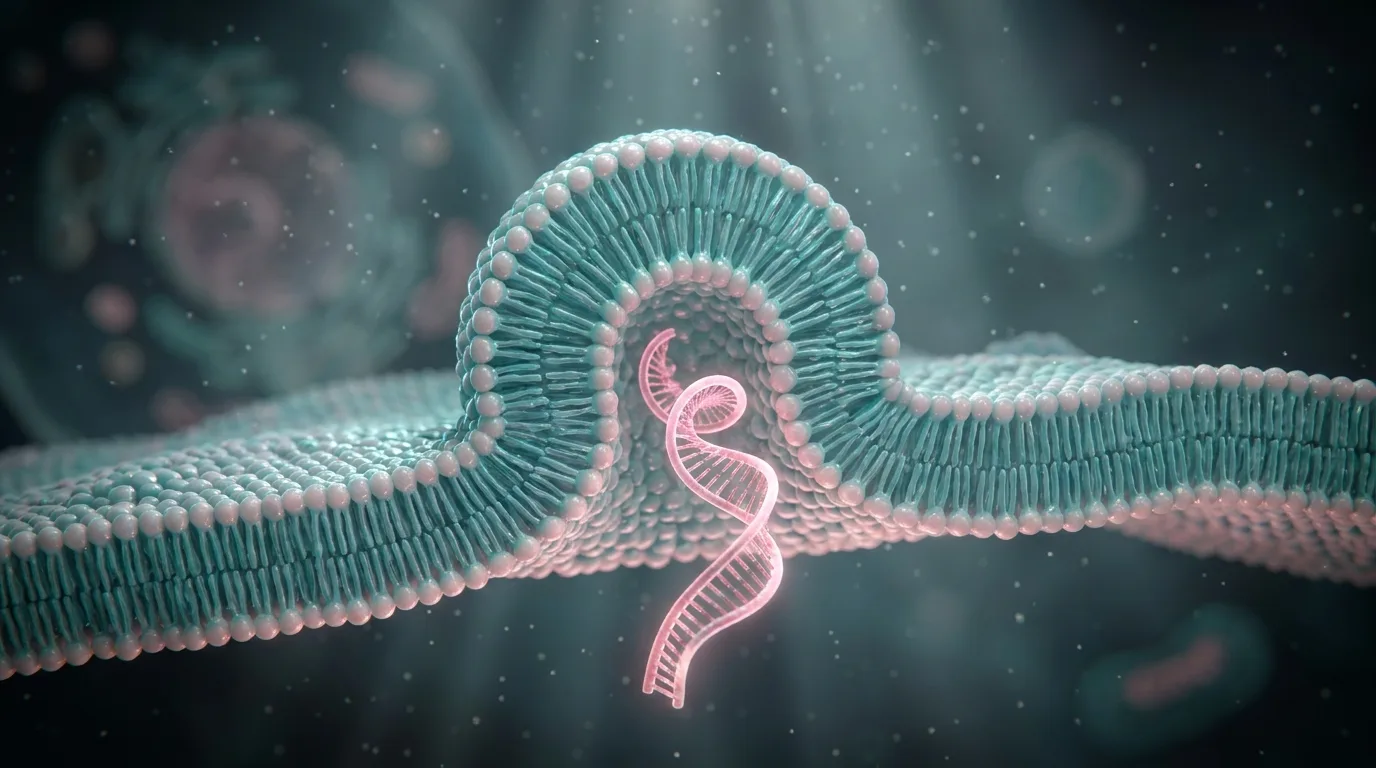
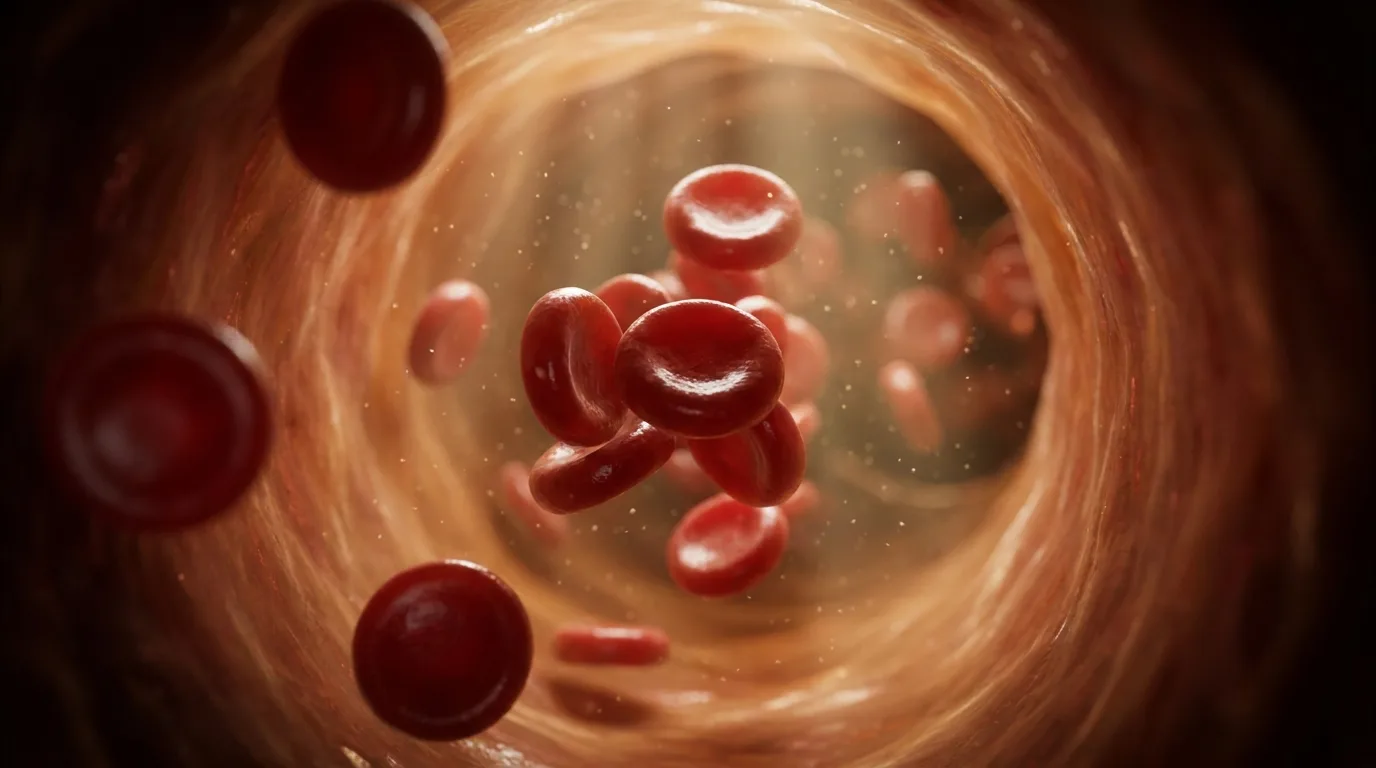
We do not render for the sake of it. Each of these needed three dimensions to be understood, because the shape or the motion was the point. Tap through them.

60+ studies, side by side: why your best science never reaches the physicians it was written for, and what the evidence says actually works instead.
Get the free report →A skeptical specialist trusts the result more when you are honest about the tool. So here is when three dimensions actually help, and when a clean flat sequence tells it faster.
The rule we hold to: the mechanism decides the format, not the budget. When 3D is the fastest way to understanding, we build it. When it is not, we say so, and we build the thing that is.
A 3D scene is an ingredient. What physicians remember is the story it sits inside: one they can explore, that adapts to who is watching. That is where the render goes to work.
The scene becomes something physicians drive. They open the part they care about and take an approved next step, right inside the science.
See PubVisual Engage →One approved mechanism, a different way in for each physician. The specialist gets the depth, the generalist gets the story. One review covers them all.
See Smart Pathways →“The first time our mechanism looked the way it does in my head.”
Send us the figure or the paper. We will show you what it becomes, where 3D earns its place and where it does not, and how physicians would explore it. On the house. No promises.
We build 3D where it makes the science clearer, then put it inside something a physician can explore. A scene on its own gets watched once. A scene they can drive, that adapts to their question, is the one they remember and act on. That is what we deliver.
When the shape or the motion is the point: structure and fit, a conformational change, a cascade over time, scale inside the cell. For most trial data, value stories, and comparisons, a clean interactive sequence lands faster and costs less. We will tell you which one your science needs.
Accurate to your source. Structures, interactions, and sequence come from the literature you approve, not an illustrator’s interpretation. Nothing on screen is a claim you have not already made. That is what lets it sit in front of a specialist.
Your approved science and the mechanism you want understood. You bring the target and the evidence. We do the heavy lifting, the mapping, the modeling, and the interactive build around it.
We will not tie it to a fixed date. You approve the core the normal way, at script, storyboard, and final animation. From there, that same approved core carries every version, so new cuts and languages do not restart the scientific review. The overall pace tracks your own review, which we plan around with you from day one.
Yes. Every element maps to an approved claim, so it is structured for MLR from the first frame and drops into your existing Veeva workflow.